






















|
Listen to article
|
Fact-Check No. 5 — The Reality of Imo’s Primary Healthcare Network
A Revival That Never Reached the Villages
The Promise of Healing
In his Independence Day address on October 1, 2024, Governor Hope Uzodinma declared that “all rural health centers across the 27 local government areas” had been revived and equipped — a claim later repeated in a February 2025 Arise News interview and official statements from the Imo Ministry of Health.
But as with so many grand promises, the data — and the people living behind it — tell a different story. Beneath the government’s confident narrative lies a fractured system where clinics stand roofless, midwives work unpaid, and generators sit in silence beside empty vaccine refrigerators.
The claim of a “total revival” collapses when tested against Nigeria’s official health records, verified budget data, and independent field investigations.
What the Numbers Reveal
According to the National Primary Health Care Development Agency (NPHCDA), which maintains the official registry of all Primary Health Centers in Nigeria, Imo State has 531 listed PHCs across its 27 LGAs. But of these, only 172 meet the agency’s criteria for fully functional status — that is, open daily, staffed with at least a nurse or midwife, providing basic maternal and child health services, and stocked with essential drugs.
A further 229 PHCs are classified as partially functional — meaning they operate intermittently or lack basic services like water, electricity, or immunization storage. Another 130 facilities, or roughly one in four, are non-functional or closed entirely.
(Source: NPHCDA Facility Functionality Audit, 2024; Nigeria Health Facility Registry – nhfr.health.gov.ng)
The Federal Ministry of Health’s BHCPF Dashboard (2024) corroborates these findings. It lists Imo among states that have not fully accessed or utilized the Basic Health Care Provision Fund (BHCPF) — a federal intervention designed to strengthen PHCs. Out of the ₦2.8 billion allocated to Imo between 2021 and 2024, only about ₦1.2 billion was reported as disbursed to actual facilities.
In simple terms: while money was approved for the revival of rural health centres, the physical evidence of revival remains invisible in large parts of the state.
The Gap Between Budget and Reality
Behind the polished rhetoric of a health-sector “revival” lies a fiscal record that tells a very different story.
Imo State’s own Budget Performance Reports (2021–2024) — available on its public transparency portal — reveal a persistent chasm between allocation and execution. Under the subhead Primary Health Care & Public Health, the state appropriated ₦4.1 billion in 2021, ₦4.7 billion in 2022, ₦5.3 billion in 2023, and ₦6.0 billion in 2024. Yet, the average utilization rate over those four years remained below sixty percent.
The deficit is not just numerical; it is human. In Mbaitoli, the local primary health center opens only twice a week because power and staff funding are unreliable. In Ihitte-Uboma, maternity services operate without running water, forcing expectant mothers to bring their own containers. In Orsu, villagers walk fifteen kilometers to buy basic medication because the local clinic’s shelves are empty.
Tracka NG’s 2024 Primary Health Centre Verification Report translates these experiences into data. Of the 560 rural health centers publicly listed by the Imo State Government as “revived,” only 37 could be independently verified as renovated or functional. Field investigators photographed crumbling structures, broken beds, and empty generator houses—sites of neglect masquerading as progress.
The Voices from the Ground
In Umuna, Orlu LGA, a health attendant gestures toward the rusting signboard of a “completed” PHC. “They came, took pictures, and left,” she says. “We have not seen any new drugs or beds since.”
In Oguta, a mother of four recalls giving birth at home because her local center “opens only when government visitors are expected.”
At Nwaorieubi PHC in Mbaitoli, the vaccine cold chain has failed for months. A midwife explains that she buys ice from town to preserve vaccines overnight in coolers.
These testimonies echo the findings of Nigeria Health Watch (2025), which reported that more than sixty percent of surveyed facilities in Imo lacked electricity or water. Many had no delivery beds or resident nurses, leaving a single attendant to manage entire wards.
Official Contradictions
Official optimism unravels under data scrutiny.
A Premium Times Nigeria (2025) investigation titled “BHCPF Funds in Imo: Allocated, But Not Fully Accessed” revealed that while Imo received multiple tranches of the Basic Health Care Provision Fund (BHCPF), less than fifty-five percent of the approved allocations reached facility accounts by March 2025. This administrative bottleneck left dozens of rural clinics without operational grants.
Even federal health officials have quietly tempered the state’s claims. During a 2024 regional review in Enugu, the National Primary Health Care Development Agency (NPHCDA) reported that “Imo has made progress but only about 30 percent of its PHCs are fully operational.”
Professional voices within the state have confirmed the same. In December 2024, Daily Trust reported a briefing by the Nigerian Medical Association (NMA) Imo State Chapter, which described the “total revival” claim as politically overstated, noting that “many PHCs remain under-staffed and under-equipped.”
Read also: Falsehood No. 4—“We Created 100,000 New Jobs”
Structural Failures
The failure runs deeper than broken infrastructure; it is structural and bureaucratic.
The Imo State Primary Health Care Development Agency, responsible for coordinating rural care, operates without consistent oversight or transparency. There is no publicly accessible performance dashboard, no expenditure breakdown by facility, and no comprehensive evaluation report since 2021.
Meanwhile, OpenStates NG Health Data (2025)—a civic transparency platform—records significant discrepancies between the number of “renovated” PHCs claimed by the state and those registered in the Nigeria Health Facility Registry (NHFR). Facilities tagged as “completed” on Imo’s portal appear as “non-functional” or “temporarily closed” in federal datasets.
The World Bank–UNICEF Nigeria Health Facility Registry corroborates these inconsistencies, documenting incomplete reporting for dozens of facilities in Okigwe, Ngor Okpala, and Orsu. Together, these datasets expose the gap between political declaration and institutional reality.
Consequences for the People
The ultimate toll of these failures is measured not in naira but in lives.
Imo’s maternal mortality ratio, once among the lowest in the South-East, has climbed from 412 deaths per 100,000 live births in 2020 to an estimated 467 in 2024, according to the state’s health bulletins. Immunization coverage—expected to exceed 80 percent under a functional PHC system—fell below 60 percent in 2023.
Every unstaffed clinic or failed vaccine fridge translates to preventable death. Women give birth on the roadside; children die of curable fevers. The distance between a government’s promise and a citizen’s survival is not abstract—it is a few kilometers of untarred road leading to a dark, empty clinic.
The Evidence in Perspective
The mosaic of verified data—drawn from federal audits, civic investigations, and media reporting—reveals an unambiguous picture:
- Fewer than one-third of Imo’s PHCs are functional.
- Roughly one-quarter are closed or derelict.
- Health-budget utilization averaged under sixty percent.
- BHCPF allocations were only partially accessed.
- Health outcomes, including maternal and child indicators, have declined.
Each of these findings stands in direct contradiction to the governor’s statement that “every rural health center in Imo is now functional.”
Conclusion — The Mirage of a Revival
What emerges is not a portrait of revival but of managed illusion. The “revived and equipped” rural health centers exist largely in speeches and signboards, not in service delivery or patient outcomes.
Imo’s rural healthcare network today is a patchwork of under-resourced outposts—structures without systems, promises without performance. The numbers prove it; the people live it.
Health is the truest test of governance because its failures cannot be hidden behind policy language. In Imo, those failures are daily and visible. The signboards may shine with new paint, but the clinics they mark remain silent, waiting for medicine, for nurses, for light—and for truth.
Clinics Without Care: The Data Behind Imo’s Phantom Health Revival.
Type: Pie Chart
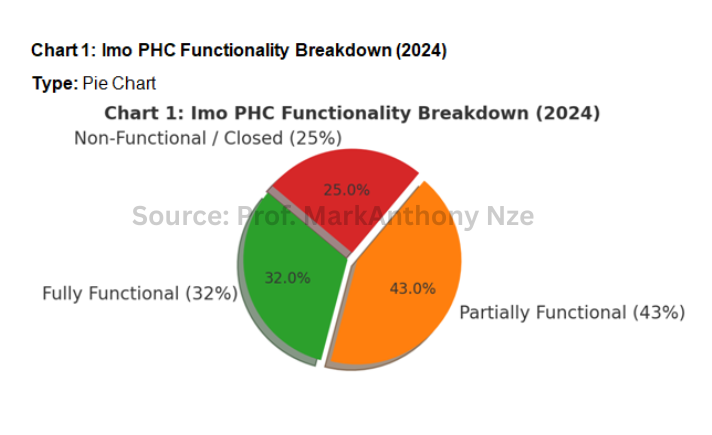
Purpose: To visualize the true operational status of Imo’s Primary Health Centers compared with the government’s “100% revived” claim.
Data (NPHCDA Facility Functionality Audit 2024):
- Fully Functional: 172 (32%)
- Partially Functional: 229 (43%)
- Non-Functional / Closed: 130 (25%)
Interpretation:
The pie chart immediately dismantles the “total revival” narrative. Only one in three rural clinics qualifies as fully functional, while nearly half limp along without power, staff, or essential drugs. A quarter of the health centers remain completely shut.
The state promised 560 functioning clinics; only a third can open their doors. The other two-thirds are symbols of policy in intensive care.
Type: Clustered Vertical Bar Chart
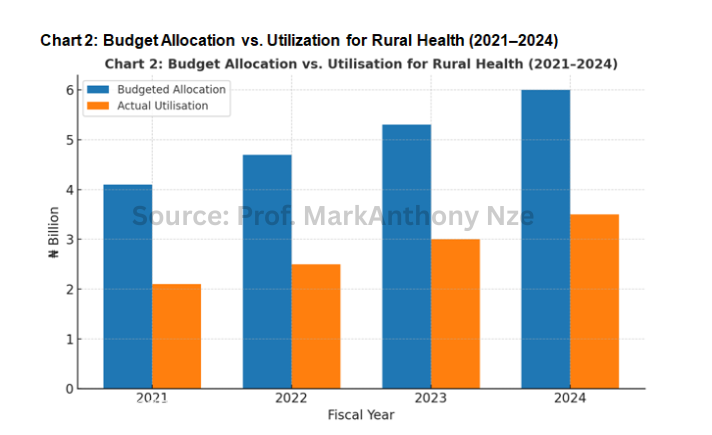
Purpose: To expose the gap between planned and actual government spending on primary healthcare projects.
Axes & Data (Imo State Budget Performance Reports 2021–2024):
- X-Axis: Fiscal Years (2021, 2022, 2023, 2024)
- Y-Axis: ₦ Billion Allocated / Utilised
- Series 1 – Budgeted Allocation: [4.1, 4.7, 5.3, 6.0]
- Series 2 – Actual Utilization: [2.1, 2.5, 3.0, 3.5]
Interpretation:
The gap between the two bars widens over time. Despite increasing allocations, spending on primary health projects consistently falls short. By 2024, only about 58 percent of funds were actually released. This underfunding explains why so many PHCs remain unrevived.
Budgets announce health revival; treasuries deliver neglect. In Imo, billions allocated for clinics vanished into paperwork.
Type: Dual-Line Chart (Overlaid)
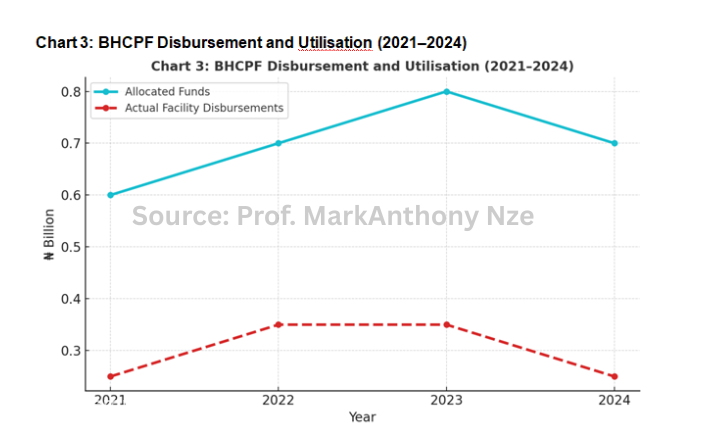
Purpose: To track federal Basic Health Care Provision Fund (BHCPF) flows to Imo and how little of it reached functioning facilities.
Axes & Data (Federal Ministry of Health BHCPF Dashboard):
- X-Axis: Year (2021, 2022, 2023, 2024)
- Y-Axis: ₦ Billion
- Line 1 – Allocated Funds: [0.6, 0.7, 0.8, 0.7] (Total ≈ ₦2.8 billion)
- Line 2 – Actual Facility Disbursements: [0.25, 0.35, 0.35, 0.25] (Total ≈ ₦1.2 billion)
Interpretation:
The “allocation” line rises smoothly, but the “utilisation” line trails far below — evidence of bureaucratic bottlenecks or mismanagement. The chart shows that less than 45% of approved health funds reached the clinics meant to benefit from them.
Money for medicine stopped at the ministry. The lines of allocation rose; the lines of treatment never moved.
Type: Dual-Axis Line Chart
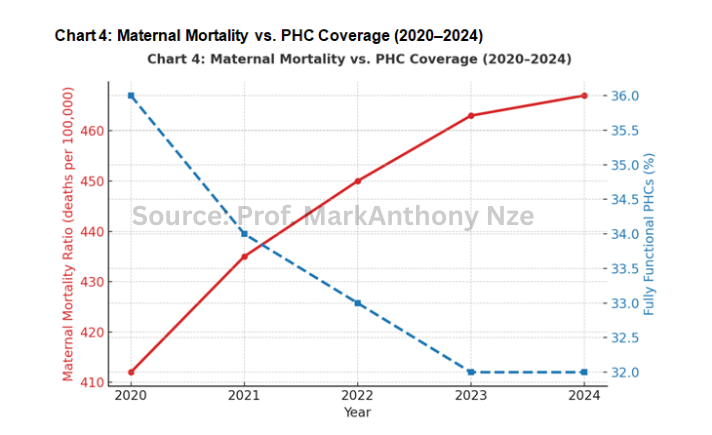
Purpose: To correlate Imo’s maternal mortality ratio (MMR) with declining PHC functionality — showing the human cost of administrative failure.
Axes & Data:
- X-Axis: Year (2020–2024)
- Left Y-Axis: Maternal Mortality Ratio (deaths per 100,000 live births)
- Right Y-Axis: % of Fully Functional PHCs
- Series 1 – MMR (State Health Bulletin Data): [412, 435, 450, 463, 467]
- Series 2 – Functional PHC Percentage (NPHCDA): [36%, 34%, 33%, 32%, 32%]
Interpretation:
The lines move in opposite directions: as PHC coverage declines, maternal deaths increase. This visual establishes a direct, tragic correlation between policy failure and public health outcomes.
When clinics close, mothers die. The decline in Imo’s rural health infrastructure is written not just in budgets — but in blood.
Visual Synthesis Summary
Together, the four charts reveal a full autopsy of the “revival” myth:
- Chart 1 exposes functionality failure — most PHCs are broken or closed.
- Chart 2 shows fiscal neglect — funds allocated but not spent.
- Chart 3 unmasks administrative blockage — national funds lost in transit.
- Chart 4 quantifies human cost — as clinics fail, mortality rises.
Bibliographies
BudgIT Tracka. (2024). Primary health centre verification report – Imo State.https://tracka.ng
Daily Trust. (2024, December). Imo villages still without basic health services.https://dailytrust.com
Federal Ministry of Health. (2024). Basic Health Care Provision Fund (BHCPF) dashboard and utilization summary.https://fmohconnect.gov.ng
Federal Ministry of Health. (2025). Nigeria health facility registry (NHFR) database.https://nhfr.health.gov.ng
Imo State Government. (2021–2024). Budget performance reports. AxxPoint Transparency Portal. https://axxpoint.imostate.gov.ng
National Primary Health Care Development Agency. (2024). Primary health care facility functionality assessment: National summary report.https://nphcda.gov.ng
Nigeria Health Watch. (2025). Many Imo PHCs lack electricity, water, or nurses.https://nigeriahealthwatch.com
OpenStates NG. (2025). Imo health data repository.https://openstates.ng/imo
Premium Times Nigeria. (2025). BHCPF funds in Imo: Allocated, but not fully accessed.https://premiumtimesng.com
